# Eyelids
# Eyelid Anatomy and Physiology
The eyelids protect the globe from injury as well as distribute the tear film.
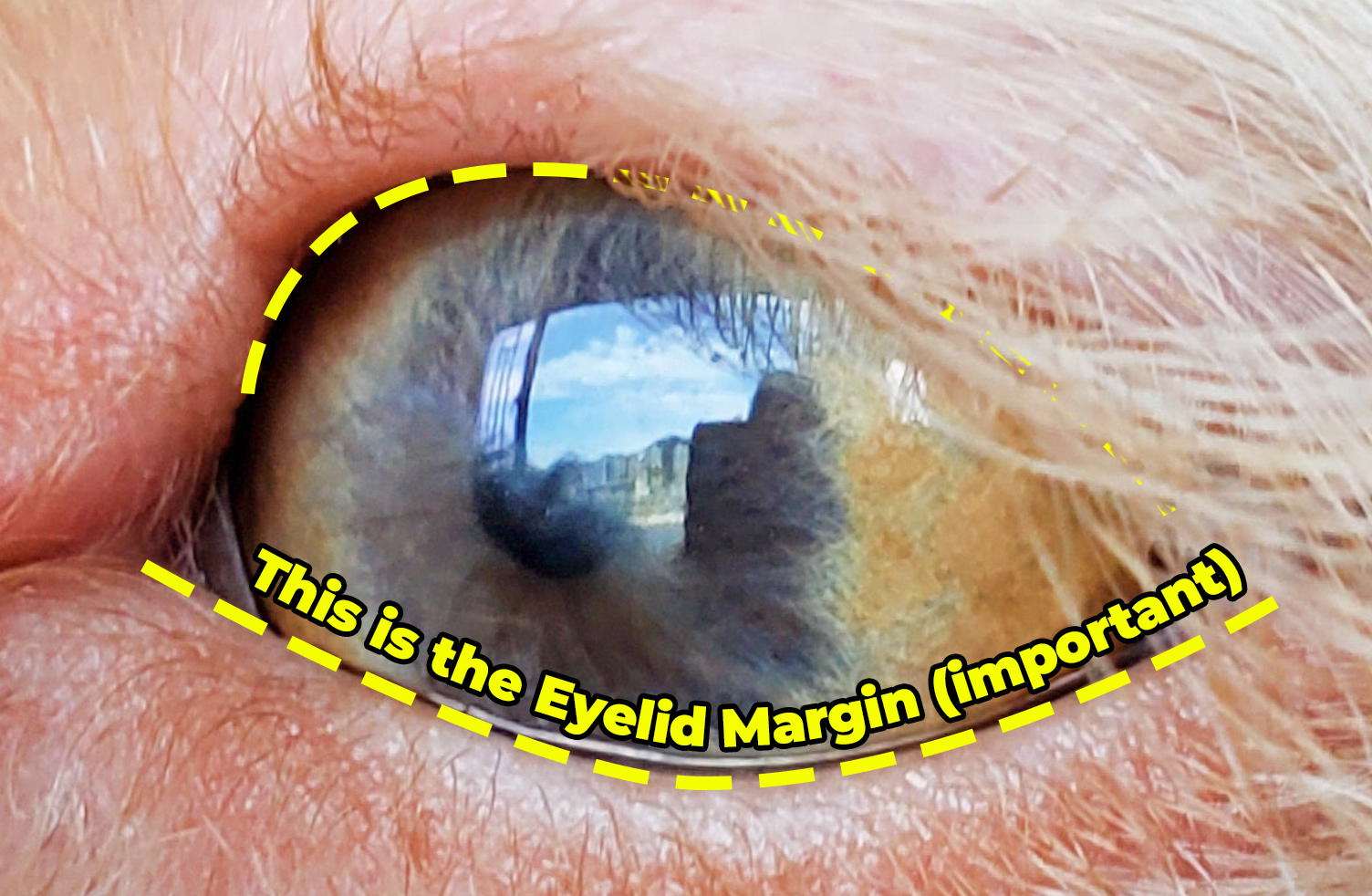
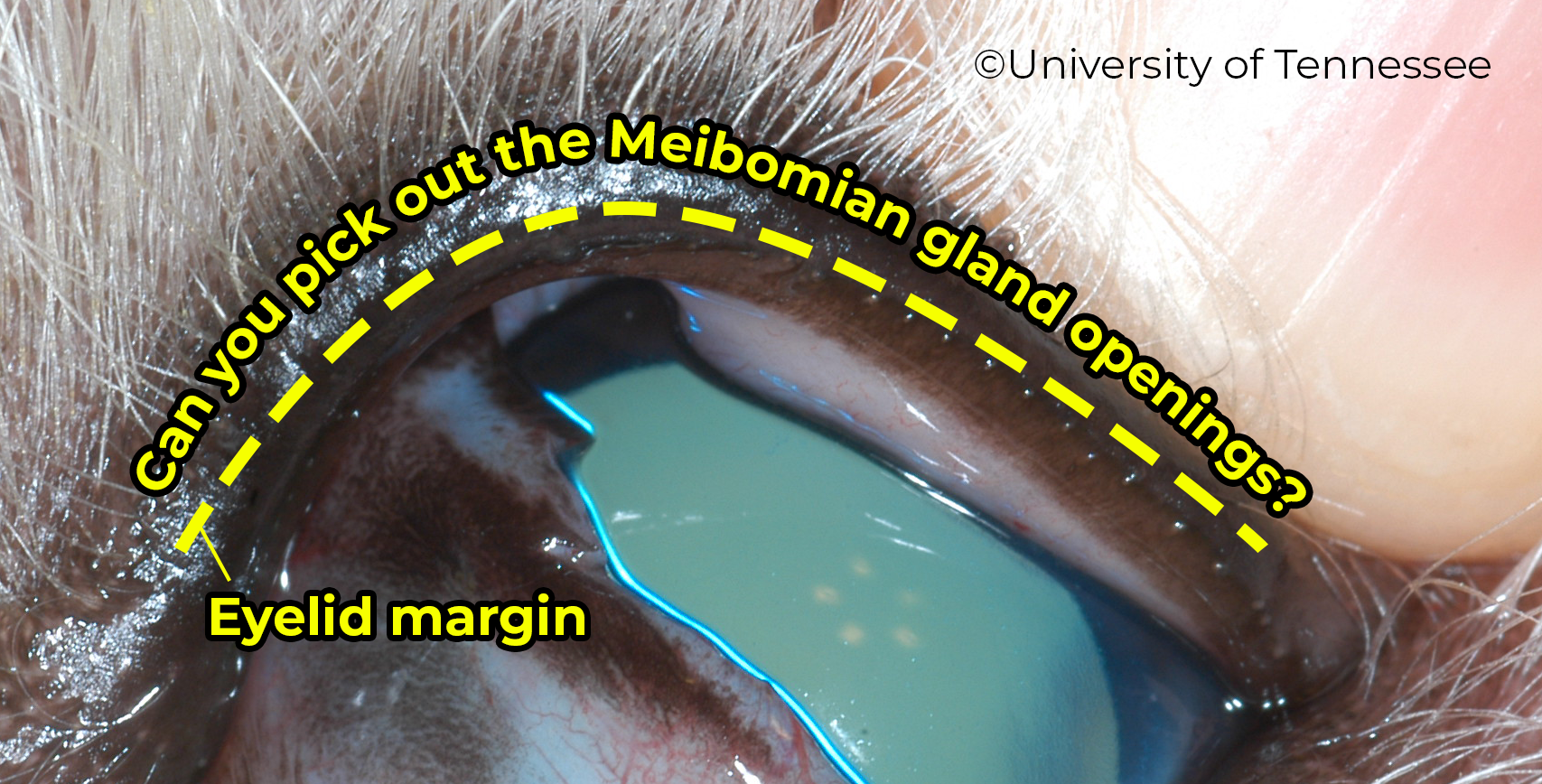
The eyelids have haired skin on the outside and are lined with conjunctiva on the inside. The eyelid margin is a special location between the skin and conjunctiva. Meibomian gland openings reside here and exude the lipid layer of the tear film. The margin gives the palpebral fissure its form and must be normal for normal eyelid function
and associated corneal health. Abnormalities in this region (the eyelid margin) such as distichia or entropion can result in corneal ulcers, keratitis, and discomfort.

# Eyelid Movement/Neurology
Closure of the eyelids is through the obicularis muscle that encircles the eyelids just under the skin. There are also a couple muscles that are involved specifically in elevating the upper eyelid (which in mammals is the most mobile eyelid) - the levator palpebrae superioris and Muller’s muscle. The latter (Muller’s) has sympathethic innervation (through CN V) and is the reason you will note ptosis (drooping of the upper eyelid) with Horner’s syndrome.
Sensation of the eyelids is done through the trigeminal nerve (CN V) although medially and laterally are innervated by different branches. Laterally it is through the maxillary branch and medially it is with the ophthalmic branch. It’s possible for a branch to be affected in isolation from the other branches so when testing a palpebral reflex, tap on both the medial and lateral aspects of the eyelids to test each branch separately and because it’s fun to tap.
Motor to the eyelids is done predominately through the facial nerve (CN VII) although the levator palpebrae muscle is through fibers branching off of CN III. Animals with facial nerve paralysis will have an absent palpebral reflex and are at risk for neuroparalytic keratitis - essentially corneal disease from exposure due to the animal’s inability to close its eyes. These animals are usually still sighted and may retract their globes and elevate their third eyelids in response to a menance response test or physically shy their heads away.
# Glands of the Eyelids
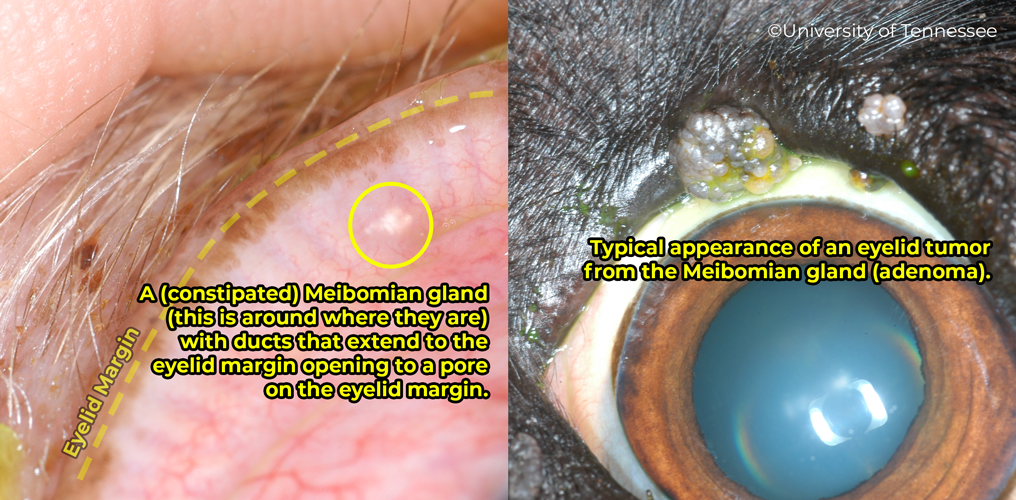
There are a few glands in and around the eyelids. The meibomian glands are the most commonly referenced gland as they produce lipid for the tear film and can be prone to development of tumors in middle-to-older aged dogs. The glands themselves lie within the eyelid a few millimeters from the eyelid margin (see image below). Their ducts open into the eyelid and are seen as small pores at the eyelid margin. These pores/openings can serve as an anatomic landmark for eyelid surgeries. When clogged (e.g. by a mass) the glandular material can build up and expand the eyelid. The lipid material is also inflammatory and can result in focal lid swelling.
The other glands lie superficially on the skin of the eyelid and produce sebaceous material or sweat.
# Normal Conformation
When examining the eyelids, pay particular attention to the eyelid margin which should rest comfortably against the cornea. If the eyelid margin cannot be appreciated then a pathologic problem may be present. Digitally manipulate the eyelid margins to more thorougly assess the position and placement as well as the underside of the eyelid.

# Ankyloblepharon
The fusion of the upper and lower eyelids. This is normal for the first 10-15 days of life in some mammals. If the eyelids open prematurely the cornea may dry as the tear glands are not completely developed. Lubricants will be needed until 2 weeks after birth.
At times infection can occur underneath the eyelids while they are still sealed. This condition is called Ophthalmia Neonatorum (see more below).
# Abnormalities of Eyelid Hairs (Cilia)
# Trichiasis
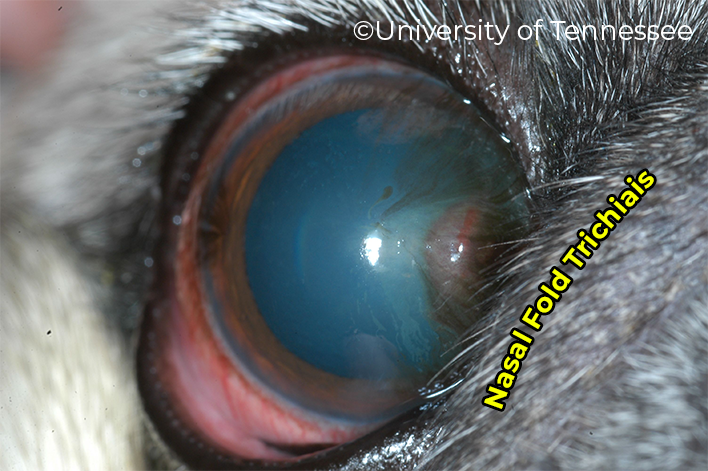
Trichiasis is when normal hair makes contact with the cornea or globe. Usually this is from prominent nasal folds (e.g. pug or English Bulldog) or from other conformational changes/abnormalities such as entropion. In some breeds (e.g. Shih Tzu) the hair can arise from a patch of skin at the medial canthus (medial trichiasis).
Treatment
- If trichiasis is secondary to entropion, correct underlying entropion with surgery (pocket medial canthoplasty for medial trichiasis, Hotz-Celsus for entropion, or facial fold resection) or temporary measures (tacking, subdermal lid filler)
# Distichia
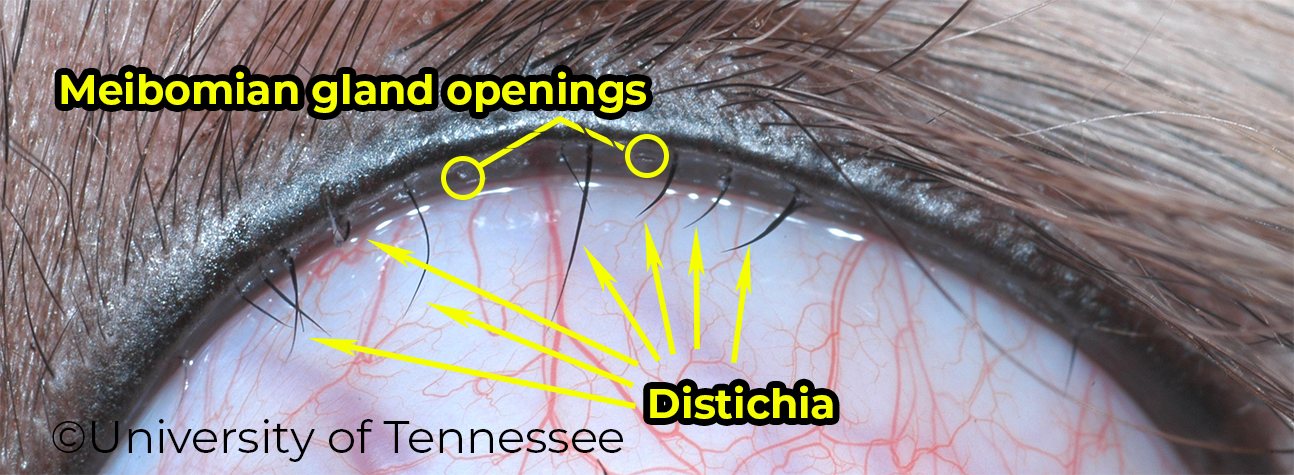
- Abnormal hairs arising from the tissue around the Meibomian glands (MG) that extend through the MG openings or pores at the eyelid margin
- Usually not problematic - many dogs will have long or many distichia without any issue or problem. However, occassionally “stout” distichia or dogs that are particularly sensitive to hairs, may exhibit discomfort, keratitis, or rarely, ulceration in the presence of distichia.
Treatment
- Plucking distichia and assessing response to distichia’s absence will help confirm they are a problem (vs like allergies).
- If distichia strongly suspected to be an issue, then can remove the hair but regrowth likely, therefore reduce chances of that occuring with either cryotherapy to terminate the hair follicle or use electrocautery.
- Surgical means of removing parts of the eyelid can also be utilized but require precise techniques to avoid significant scarring to the lid margin.
# Ectopic Cilia
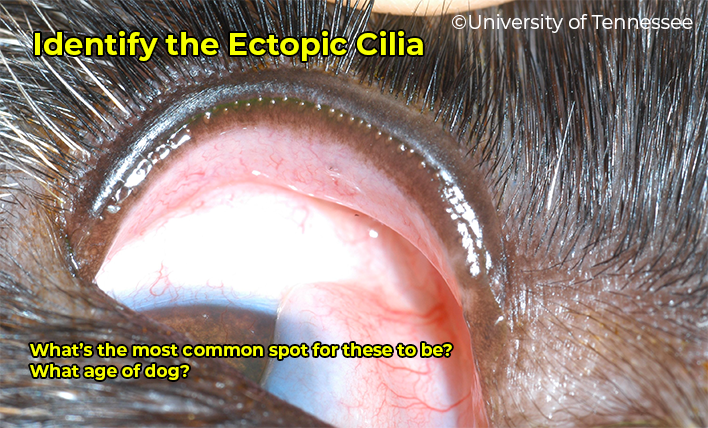
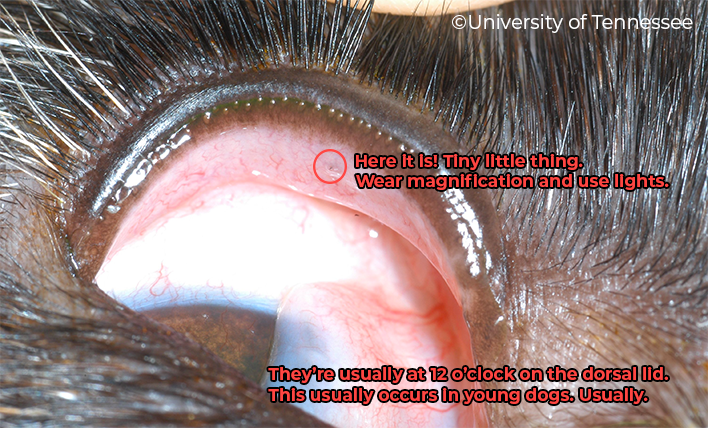
- Abnormal hairs arising from the tissue around the Meibomian glands (MG) that extend through the conjunctiva on the bulbar side of the eyelid
- Usually causes a problem; be most suspicious in young dogs with persistent blepharospasm or ulcers or keratitis focused on the dorsal aspect of the cornea (closest to the dorsal lid)
Treatment is sugical removal (en bloc resection) with cryotherapy potentially to prevent regrowth of ectopic cilia.
# Abnormalities of Eyelid Conformation
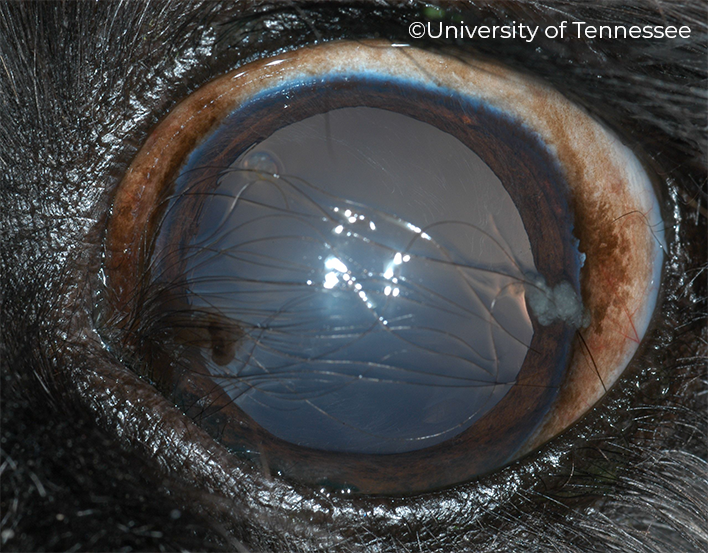
# Ectropion

- Note the exposure of the conjunctiva and the little "pocket" that forms as a result of the eversion.
- This particular conformation with the lid so ectropic it forms kind of a diamond shape is sometimes called a "pagoda" lid by people who want to sound cool and give the abnormality an oriental kind of flavor.
- Other forms of ectropion may not necessarily have this diamond shape.
- Eversion of eyelid seen in Bloodhounds, Bassetts, Cockers, St. Bernards, or unfortunately, in over-corrected entropion surgeries
- Clinical signs include gross eversion of eyelid, chronic conjunctivitis, ocular discharge, +/- keratitis.
- Underlying primary cause is usually excessive lid length or lid laxity
Treatment
- None is usually needed unless keratitis is present
- Medical: Intermittent flushing or lubrication & topical corticosteroids
- Surgery: Lid shortening (wedge resection) alone or in combination with lid “strengthening” techniques to help with lid laxity
# Entropion
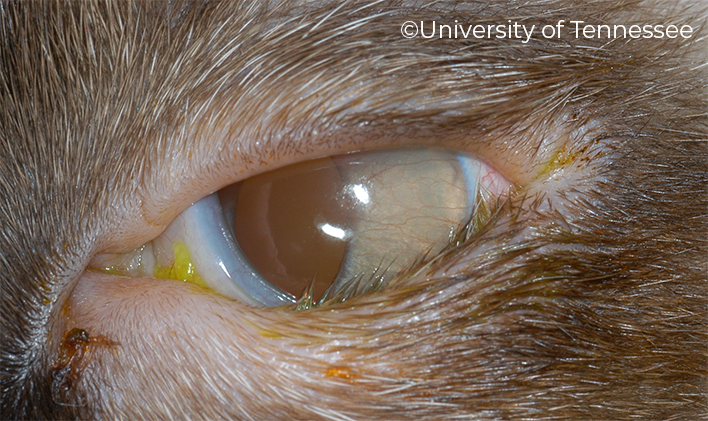
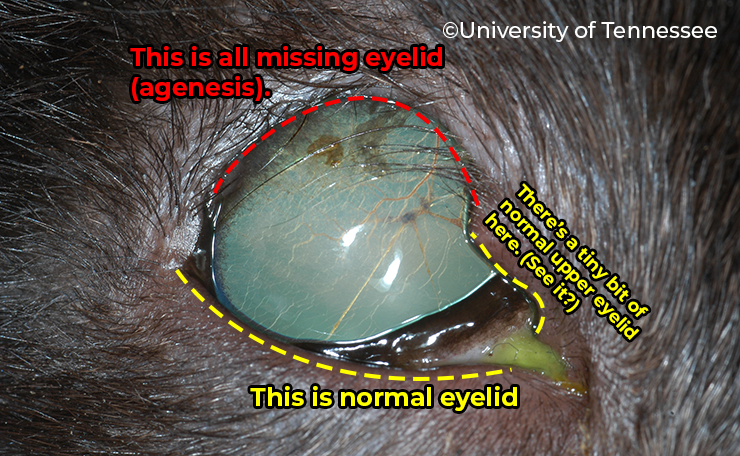
- Note the normal upper lid where the lid margin is clearly visible
- The lateral 2/3rd (or more) are rolled in (no visible margin because it's rolled in) and the hairs are physically connecting with the cornea (trichiasis) resulting in...
- Keratitis (that's the other thing) as evidenced by neovascularization in the lateral half or so of the visible cornea
- When diagnosing entropion, look for supporting evidence with keratitis or ulcers in the suspected region
- Entropion is rolling in of the eyelid, likely with trichiasis and (ulcerative) keratitis to follow
- Causes of entropion include:
- Congenital (e.g. Sharpei) or developmental (puppy)
- Cicatricial (from scarring, say from an unrepaired eyelid laceration)
- Spastic - when intense squinting results in rolling in of the eyelid
- To diagnose spastic entropion, place a drop of proparacaine into the affected eye and assess whether conformation of the lid returns to “normal” (may have to flip out and play with the lid to see how it goes)
- If the lid stays entropic, then you have a more permanent problem
- Clinical signs include ulcerative or nonulcerative keratitis in the region of entropion, chronic conjunctivitis, discharge.
Treatment
- Depends on the type or cause of the entropion
- The author usually thinks of entropion treatment in terms of 2 large categories:
- Entropion that will most likely get better with time (puppy entropion) or with resolution of the primary cause (i.e. spastic entropion that resolves after an ulcer heals)
- For puppy entropions, the entropion should be temporarily corrected by temporarily tacking the eyelid down or maybe with a collagen injection if the entropion is mild-moderate
- For spastic entropions, temporary tack the eyelid and allow the “painful” pathology of the eye resolve (e.g. ulcer heal). Remove sutures when confident dog is comfortable.
- Entropion that will not get better with time
- These cases require surgical correction - with Hotz Celsus or comparable surgical technique
- Entropion that will most likely get better with time (puppy entropion) or with resolution of the primary cause (i.e. spastic entropion that resolves after an ulcer heals)
# Other Eyelid-Related Conditions
# Lagophthalmia
- Lagophthalmia is failure to blink completely.
- Sometimes due to facial nerve paralysis, but more commonly seen in brachycephalics as a conformational problem.
- The orbits in these dogs are so shallow that the eyeballs protrude anteriorly – so-called “physiologic exophthalmos.”
Treatment (if necessary)
- Medial canthoplasty.
- A surgical procedure that shortens the palpebral fissure.
- In short, the nasal few mm of the superior and inferior lids are freshened and sutured together.
- By shortening the palpebral fissure each blink covers more of the cornea, thus reducing the lagophthalmia.
- As an added bonuses this procedure also eliminates medial canthal entropion and medial aberrant dermis.
# Medial aberrant dermis
Small breeds often have a small piece of dermis in the medial canthus of the eye, and hairs often emanate from this piece of dermis. Due to their location, these hairs can irritate the nasal aspect of the cornea leading to pigmentation, but they are often asymptomatic if they are the only ocular abnormality.
Treatment
- Benign neglect usually (cannot trim them away at the groomers unless they are super brave and anyway they’ll just regrow)
- Medial canthoplasty
# Ophthalmia neonatorum

- Infection (usually staph) under fused lids prior to the lids opening.
- Lids are swollen, a purulent exudate may be evident
- Affected puppies or kittens are usually older than 14 days (past the point of where their eyelids should open)
Treatment
- Warm compresses are placed, the lid margin is split carefully with blunt scissors and the conjunctiva is flushed
- Check for ulcers
- Treat with topical antibiotic based on culture and sensitivity
# Eyelid masses

Neoplasia
- > 90% of eyelid margin tumors are benign
- The most common are adenomas arising from the Meibomian glands (see top row in above image for examples)
- Papillomas and melanomas can also be seen, both of which also behave relatively benignly
- More rarely, malignancies such as mast cell tumor, squamous cell carcinoma, hemangiosarcoma, and fibrosarcoma will be encountered
- The main problem induced by the benign tumors is that if they get large enough they will interfere with lid function, induce keratitis and conjunctivitis from rubbing on the ocular surface, and sometimes cause superficial ulcers (also from abrading the cornea)
Diagnosis
- Biopsy with histopathology is the only sure way to diagnose the specific type of tumor present
- That said, many pedunculated “cauliflower” type masses arising from the eyelid margin or in the area of the Meibomian/tarsal glands are presumed to be Meibomian gland adenomas or epitheliomas and can be treated conservatively (i.e. probably will not need for aggressive wide resection)
- More “expansile” masses within the eyelid tissue itself should be examined carefully on the “underside” of the eyelid to look for a chalazion or aspirated for cytology to rule out rarer conditions like mast cell tumor
Treatment
- The author usually approaches most suspected benign eyelid masses (i.e. Meibomian gland adenomas) in one of a few ways:
- Conservative: “Wait and see” - some masses will not necessarily be causing keratitis or conjunctivitis. Owners should be warned that rapid growth is possible and small masses are more easily treated than large ones
- Surgical:
- “Snip and Freeze” - the author’s colloquial way of saying debulking and cryotherapy of an eyelid mass
- The tumor is first trimmed down to the eyelid margin doing as much to not disrupt the margin of the eyelid
- A currette or similar instrument (e.g. tips of scissors, 11 blade, etc.) is used to remove any inspisated gland material or neoplasia
- The cryo probe is placed in the bed of the debulked tumor and 2 or 3 fast-freeze-slow-thaw cycles are applied
- The freezing is applied until an “ice ball” forms around the affected area and extends ~3-5 mm beyond those margins
WARNING
When applying cryotherapy, over the counter “wart” remedies do not typically get to the level of cold needed for lysis of neoplastic cells. You want a temperature around or colder than -20 to -40°C; N2O (nitrous) cryo gets to -25°C
- Eyelid resection
- 1/3 of the eyelid margin can safely be removed without decreasing function.
- If >1/3 of the margin needs to be removed, then blepharoplastic procedures need to be done.
- For small tumors a wedge resection or pentagonal excision is done.
- The details of how to perform a wedge resection can be found in the “Surgical Techniques” notes as well as in texts. Accurate closure of the margin with the figure-8 suture is of utmost importance to prevent postoperative corneal irritation and/or ulceration.
- “Snip and Freeze” - the author’s colloquial way of saying debulking and cryotherapy of an eyelid mass
Chalazion 
- Granulomatous inflammation of the tarsal gland/glands.
- Localized mass beneath conjunctival surface, middle-aged dogs.
- Treatment
- Warm compresses, topical antibiotics/dex, lance the chalazion through a small incision on conjunctiva
# Eyelid lacerations
Because of the tremendous blood supply, only minimal debridement should be done if at all. Immediate repair is a necessity to prevent tissue loss. Place the figure-8 margin suture first. Two layer closure is needed for long lacerations. Make sure no sutures penetrate the conjunctiva.
← Orbit Nasolacrimal →